Understanding the correct leads ecg placement is essential for accurate cardiac diagnostics. A small error can lead to misdiagnosis, delayed treatment, or unnecessary tests. Let’s dive into the science, standards, and secrets behind perfect ECG lead positioning.
What Is Leads ECG Placement and Why It Matters

Leads ecg placement refers to the precise positioning of electrodes on the body to record the heart’s electrical activity. These electrodes capture voltage differences over time, generating the familiar ECG waveform. Incorrect placement can distort the waveform, leading to false interpretations.
The Science Behind ECG Leads
An electrocardiogram (ECG or EKG) measures the heart’s electrical impulses through 12 standard leads. These leads are derived from 10 electrodes placed on the limbs and chest. Each lead offers a unique ‘view’ of the heart’s electrical activity, allowing clinicians to assess rhythm, conduction, ischemia, and infarction.
- Standard 12-lead ECG uses 4 limb electrodes and 6 precordial chest electrodes.
- Each lead represents a specific anatomical region of the heart.
- Incorrect placement alters vector direction, affecting diagnosis.
According to the American Heart Association (AHA), even a 2 cm displacement of a precordial lead can significantly alter ECG readings, mimicking conditions like myocardial infarction.
Common Misconceptions About Lead Placement
Many healthcare providers assume that approximate placement is sufficient. However, research shows that up to 50% of ECGs have at least one lead misplaced. Some believe that modern machines can ‘correct’ for poor placement, but this is a dangerous myth.
- Myth: ‘The machine compensates for errors.’
- Reality: Algorithms interpret signals as given; they don’t fix misplacement.
- Myth: ‘Chest leads don’t need to be exact.’
- Reality: V1 and V2 placement is critical for detecting anterior infarcts.
‘Accurate lead placement is the foundation of a reliable ECG. No algorithm can replace proper technique.’ – Journal of Electrocardiology
Standard Guidelines for Leads ECG Placement
Adhering to standardized protocols ensures consistency and diagnostic accuracy. The most widely accepted guidelines come from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology.
Limb Lead Placement: Arms and Legs
Limb leads (I, II, III, aVR, aVL, aVF) are derived from electrodes placed on the arms and legs. While traditionally placed on the limbs, modern practice often places them on the torso to reduce motion artifact, especially during stress tests.
- Right Arm (RA): Upper right chest or right shoulder area.
- Left Arm (LA): Upper left chest or left shoulder area.
- Right Leg (RL): Lower right abdomen (ground electrode).
- Left Leg (LL): Lower left abdomen.
When placing limb electrodes on the torso, ensure they are at the same horizontal level to avoid baseline drift. The American College of Cardiology emphasizes that asymmetrical placement can cause axis deviation artifacts.
Precordial (Chest) Lead Placement: V1 to V6
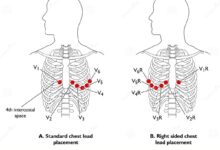
The chest leads (V1–V6) provide a horizontal view of the heart and are crucial for diagnosing anterior, lateral, and septal myocardial infarctions.
- V1: 4th intercostal space, right sternal border.
- V2: 4th intercostal space, left sternal border.
- V3: Midway between V2 and V4.
- V4: 5th intercostal space, midclavicular line.
- V5: Same horizontal level as V4, anterior axillary line.
- V6: Same level as V4 and V5, midaxillary line.
Incorrect V4 placement is one of the most common errors. Placing it too high or too lateral can mask signs of infarction. A study in Circulation found that 30% of ECGs had V4 misplaced by more than one intercostal space.
Common Errors in Leads ECG Placement
Despite clear guidelines, errors in leads ecg placement are alarmingly common. These mistakes can lead to false positives, missed diagnoses, and unnecessary interventions.
Reversal of Limb Electrodes
One of the most frequent errors is the reversal of right and left arm electrodes. This causes lead I to invert, and leads II and III to swap, resulting in apparent right axis deviation and pseudo-infarct patterns.
- Signs of limb lead reversal: Negative P wave in lead I.
- Lead aVR shows upright P and QRS complexes.
- Can mimic dextrocardia or posterior MI.
Automated ECG machines may not flag this error, making visual inspection essential. The European Society of Cardiology recommends always checking lead I for a positive P wave in normal sinus rhythm.
Incorrect Precordial Lead Positioning
Misplacing chest leads, especially V1 and V2, is common in obese or muscular patients. V1 placed in the 3rd or 5th intercostal space can mimic arrhythmias or bundle branch blocks.
- V1 too high: May mimic right bundle branch block (RBBB).
- V1 too low: Can obscure right ventricular hypertrophy signs.
- V4 misplaced laterally: May miss anterior ST elevation.
A 2020 study in The American Journal of Emergency Medicine found that 42% of emergency department ECGs had at least one precordial lead incorrectly placed.
‘A misplaced lead is not just a technical flaw—it’s a clinical risk.’ – Dr. Emily Thompson, Cardiologist
Special Considerations in Leads ECG Placement
Certain patient populations and clinical scenarios require modifications to standard leads ecg placement to ensure diagnostic accuracy.
leads ecg placement – Leads ecg placement menjadi aspek penting yang dibahas di sini.
ECG in Women: Breasts and Lead Positioning
In women, breast tissue can interfere with proper electrode contact. The standard recommendation is to lift the breast and place V3, V4, V5, and V6 on the chest wall, not on the breast tissue.
- V4 should still be placed in the 5th intercostal space at the midclavicular line, regardless of breast size.
- Failure to adjust leads can lead to inferior displacement of lateral leads, mimicking old infarcts.
- Use of adhesive pads or extra gel may improve contact.
A study published in Heart Rhythm showed that 60% of ECGs in women had lateral leads placed too low due to breast tissue interference.
ECG in Obese or Muscular Patients
In obese patients, standard anatomical landmarks may be difficult to palpate. In muscular individuals, pectoral muscles can distort signals.
- Use bony landmarks (sternal angle, clavicle) as reference points.
- Consider ultrasound guidance in extreme cases.
- Document any deviations from standard placement.
For very large patients, some clinicians use alternative lead placements like the ‘high intercostal’ or ‘horizontal’ method, though these are not universally accepted.
Alternative Lead Placements and Their Uses
While the 12-lead ECG is standard, alternative lead configurations are used in specific clinical situations to enhance diagnostic yield.
Right-Sided ECG (V1R to V6R)
Right-sided leads are used to detect right ventricular infarction, often associated with inferior wall MI.
- V1R: 4th intercostal space, right sternal border (same as V1).
- V2R: 4th intercostal space, right midclavicular line.
- V3R to V6R: Continue across the right chest.
ST elevation in V4R is a key indicator of right ventricular involvement. The sensitivity increases when leads are placed within 10 minutes of symptom onset.
Posterior ECG (V7 to V9)
Posterior leads help diagnose posterior myocardial infarction, which may not be visible on standard leads.
- V7: 5th intercostal space, left posterior axillary line.
- V8: 5th intercostal space, left mid-scapular line.
- V9: 5th intercostal space, left paraspinal area.
Posterior MI often shows reciprocal changes in V1–V3 (tall R waves, ST depression). Adding V7–V9 can confirm the diagnosis.
‘Posterior leads are underutilized but can be lifesaving in diagnosing hidden infarcts.’ – Journal of the American College of Cardiology
Training and Quality Control in Leads ECG Placement
Despite its simplicity, ECG lead placement requires proper training and ongoing quality assurance to maintain diagnostic accuracy.
Importance of Proper Training
Nurses, EMTs, and technicians are often responsible for ECG acquisition. However, training varies widely across institutions.
- Many programs provide only 1–2 hours of ECG lead instruction.
- Hands-on practice with feedback is often lacking.
- Refresher courses are rarely mandated.
A 2019 survey by the American Association of Nurse Practitioners found that only 38% of primary care providers felt confident in their ability to place ECG leads correctly.
Implementing Quality Assurance Programs
Hospitals and clinics should implement regular audits of ECG tracings to identify placement errors.
- Review random ECGs monthly for lead accuracy.
- Use visual checklists during acquisition.
- Provide feedback and retraining when errors are found.
Some institutions use AI-assisted tools to flag potential lead reversals or misplacements before the ECG is interpreted.
Technological Advances in Leads ECG Placement
Emerging technologies aim to reduce human error and improve the accuracy of leads ecg placement.
Smart Electrodes and Wearable Sensors
New electrode designs include built-in sensors that detect position and contact quality.
leads ecg placement – Leads ecg placement menjadi aspek penting yang dibahas di sini.
- Some systems use Bluetooth to alert technicians if a lead is misplaced.
- Wearable ECG vests with pre-positioned electrodes reduce setup time and errors.
- Used in ambulatory monitoring and stress testing.
Companies like AliveCor and Zio have developed FDA-approved wearable ECG devices that minimize placement variability.
AI and Machine Learning in ECG Interpretation
Artificial intelligence is being trained to detect lead placement errors automatically.
- AI algorithms can identify limb lead reversals with >95% accuracy.
- Some systems analyze P-wave morphology across leads to flag inconsistencies.
- Still in development for widespread clinical use.
A 2021 study in Nature Medicine demonstrated an AI model that could detect incorrect precordial lead placement by analyzing QRS amplitude patterns.
‘Technology won’t replace the clinician, but it can catch the mistakes we miss.’ – Dr. Rajiv Patel, Biomedical Engineer
Why is leads ecg placement so prone to error?
Leads ecg placement is prone to error due to reliance on anatomical landmarks that can be difficult to identify, especially in obese, edematous, or muscular patients. Time pressure in clinical settings, inadequate training, and lack of standardized protocols also contribute. Even small deviations—just one intercostal space—can alter ECG interpretation significantly.
What happens if ECG leads are placed incorrectly?
Incorrect leads ecg placement can lead to misdiagnosis, such as false ST-segment elevation (mimicking heart attack), axis deviation, or bundle branch block patterns. It may result in unnecessary interventions like thrombolytics or angiography, or conversely, missed diagnoses of acute coronary syndrome.
How can I verify correct lead placement?
Always check for expected waveforms: upright P waves in leads I, II, and aVF; negative P in aVR; R wave progression from V1 to V6. Use anatomical landmarks carefully, and consider using a placement guide or template. Visual inspection and staff training are key. Some modern ECG machines include lead placement verification features.
Are there alternatives to standard 12-lead ECG?
Yes, alternatives include right-sided ECG (V1R–V6R) for right ventricular infarction, posterior leads (V7–V9) for posterior MI, and esophageal leads for atrial activity. Wearable single-lead ECGs (like Apple Watch) are used for rhythm monitoring but are not diagnostic for ischemia.
Can AI fix bad ECG lead placement?
No, AI cannot ‘fix’ bad lead placement. While AI can detect certain errors (like limb lead reversal), it cannot reconstruct accurate data from misplaced electrodes. Prevention through proper training and technique remains the gold standard.
Accurate leads ecg placement is not just a technical detail—it’s a cornerstone of cardiac diagnosis. From understanding the anatomy to avoiding common errors and embracing new technologies, every step matters. By following standardized guidelines, investing in training, and utilizing quality control, healthcare providers can ensure reliable, life-saving ECG interpretations. Never underestimate the power of a correctly placed electrode.
leads ecg placement – Leads ecg placement menjadi aspek penting yang dibahas di sini.
Further Reading: